
Diagnosis of AAT Deficiency According to Italian Recommendations and a Clear Algorithm for Practice
Alpha-1 antitrypsin deficiency (AATD) is a genetic disorder that primarily affects the lungs and liver. It is considered a rare disease, but it is also significantly underdiagnosed. Given the availability of specific treatment, which involves the administration of purified alpha-1 antitrypsin (AAT) derived from human plasma in patients with COPD due to AATD, identifying these patients is crucial. We summarize the recently issued Italian recommendations for the diagnosis of AATD and place them in the context of Czech standards.
Introduction
Italian authors have created a detailed algorithm for the care of patients with AATD. The most challenging part is the initial detection, which falls on the shoulders of general practitioners. Therefore, they should be sufficiently informed about this disease and its diagnostic procedures.
AATD Diagnostic Algorithm
First-Level Examination
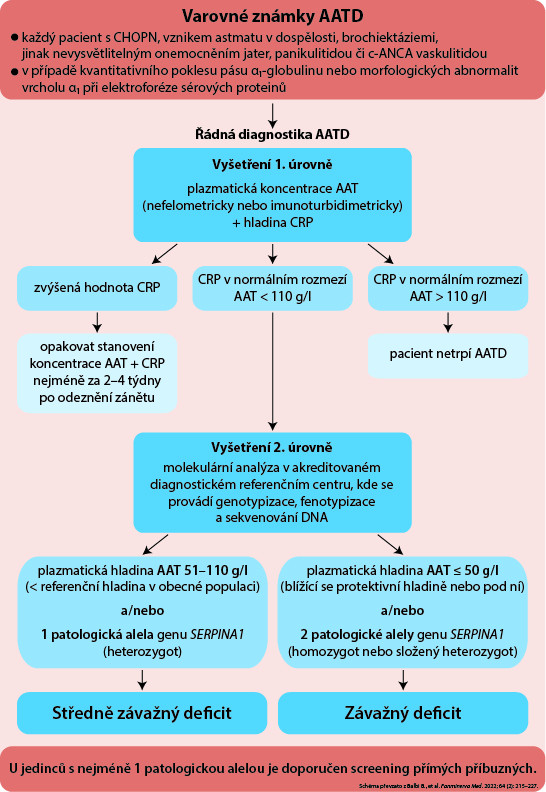
Basic screening for AATD should be conducted in every patient with COPD, adult-onset asthma, bronchiectasis, unexplained liver disease, panniculitis, or c-ANCA vasculitis.
First-level examination includes determining the level of AAT in the blood. This test can be ordered by any doctor. It is conducted using nephelometry or immunoturbidimetry with the same reliability. However, AAT is an acute-phase protein that can be elevated in cases of inflammation, infection, or injury. Therefore, it is necessary to simultaneously determine C-reactive protein (the most commonly used indicator of ongoing inflammation).
If a high level of CRP is detected, the AAT + CRP test should be repeated 2–4 weeks after the inflammation subsides. If inflammation is ruled out by a normal CRP level, a normal AAT level is > 110 mg/dl (according to Czech recommendations, the threshold is 1 g/l, i.e., 100 mg/dl).
Second-Level Examination
In patients with a normal CRP level and an AAT level ≤ 110 mg/dl (≤ 1 g/l in the Czech Republic), the second level of the diagnostic process involves phenotyping, genotyping, and DNA sequencing. This examination is conducted in accredited reference centers.
Since the risk of COPD shows an inverse correlation with AAT levels, patients with AATD were divided into 2 categories based on severity:
- Moderate severity: AAT level 51–110 mg/dl or the presence of 1 pathological allele of the SERPINA1 gene (in the Czech Republic, a level of 0.5–1 g/l is considered a mild deficiency).
- High severity: AAT level ≤ 50 mg/dl or the presence of 2 pathological alleles of the SERPINA1 gene (in the Czech Republic, an AAT level < 0.5 g/l means a severe deficiency).
Procedure for Identifying Individuals with AATD
When identifying an individual with AATD (with moderate or high severity), it is recommended to examine all direct relatives.
For all patients with AATD, consultation in a specialized center and monitoring is recommended. For patients with high severity AATD, specific treatment is considered based on additional criteria.
(zza)
Sources:
1. Balbi B., Benini F., Corda L. et al.; IDA Group. An Italian expert consensus on the management of alpha1-antitrypsin deficiency: a comprehensive set of algorithms. Panminerva Med 2022 Jun; 64 (2): 215–227, doi: 10.23736/S0031-0808.22.04592-X.
2. Chlumský J. Standard for the diagnosis and treatment of patients with COPD with proven alpha-1 antitrypsin deficiency (AATD). Česká pneumologická a ftizeologická společnost ČLS JEP, 2019. Available at: www.pneumologie.cz/upload/1583105752.959.pdf
YOU CAN ALSO DOWNLOAD THE DIAGNOSTIC SCHEME HERE IN PDF FORMAT.
Did you like this article? Would you like to comment on it? Write to us. We are interested in your opinion. We will not publish it, but we will gladly answer you.